Osseous Grafts or “Bone Grafts”
Bone loss in the jaws and around the teeth can be the result of missing teeth, periodontal disease, or trauma. This bone loss is more than a detriment to oral health and function; it can also alter facial appearance as the support for the natural contours of the face is diminished.
When a tooth is extracted, the natural stimulation to the underlying bone that is generated by the forces of biting or chewing is lost. The fact of the matter is that bone width can be reduced by as much as 25% in the first year following tooth loss.
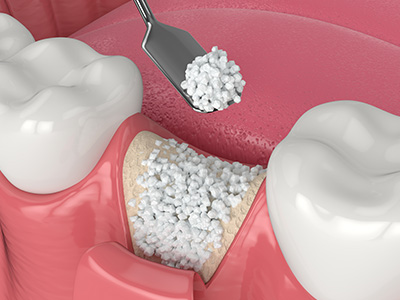
By performing grafting procedures, the oral and maxillofacial surgeon can help restore the bone to its original dimensions to maintain facial esthetics, repair the damage caused by periodontal disease as well as facilitate the success of procedures such as the placement of dental implants. A bone graft provides a platform or “scaffolding” for new bone growth and the material for a bone graft can be derived from the patient, other donor sources or be comprised of synthetic, bone-like materials.
A bone graft can be placed immediately upon the extraction of a tooth or some time after tooth loss. Placing a bone graft at the time of tooth removal reduces the amount of bone loss in the area to maintain the hard tissue support that is required for the future placement of a dental implant. When a bone graft is placed awhile after tooth loss, a separate surgical procedure is required to reflect the soft tissue, expose the underlying bone, place a graft and then suture the soft tissue back into place.
For patients lacking a sufficient amount of bone for a dental implant to replace a maxillary back tooth (upper back tooth), a procedure, which is known as a “sinus lift” is performed. During this surgical procedure, the sinus membrane is lifted, and bone graft material is added between the jaw and the floor of the sinus to provide the needed bone height to support a dental implant successfully.
In addition to bone grafting for purposes of ridge preservation or augmentation to allow for dental implants, an aesthetic ridge augmentation procedure to restore the natural contours of the bone is sometimes performed in preparation for fixed bridgework to achieve a more cosmetically pleasing result.
To guide tissue regeneration as well as protect the graft and promote healing, the oral and maxillofacial surgeon may place specialized membranes and biologically active materials over the grafting material.


A bone graft is a surgical procedure that places material where jawbone is deficient to restore lost volume and support. In dentistry, grafts create a stable foundation for tooth replacement, preserve facial contours, and repair defects caused by disease or trauma. The graft material acts as a scaffold that encourages the body to grow new, healthy bone in the treated area.
Bone grafting can be part of restorative, periodontal, or implant treatment plans and is tailored to the specific clinical need. Surgeons select graft type and technique based on the size and location of the defect, the patient’s health, and long-term treatment goals. When planned and performed appropriately, grafts improve both function and esthetics by reestablishing bone height and width.
Bone loss in the jaw most commonly results from tooth loss, untreated periodontal (gum) disease, and traumatic injury. After a tooth is removed the mechanical stimulation that maintains bone is lost, which can lead to rapid resorption; studies show significant reduction of ridge width in the first year after extraction. Chronic infection from periodontal disease also destroys the bone that supports teeth, leading to mobility and eventual tooth loss if left untreated.
Other contributing factors include systemic health conditions, prolonged tooth absence without replacement, and certain medications that affect bone metabolism. Early diagnosis and targeted treatment help slow or reverse localized bone loss and improve outcomes for subsequent restorative procedures. Regular dental exams and radiographs are important for detecting bone changes before they become extensive.
A bone graft is often necessary when there is insufficient bone volume or density to securely support a dental implant. Inadequate bone can result from long-term tooth loss, periodontal disease, or anatomic limitations such as the proximity of the sinus or inferior alveolar nerve. Restoring adequate bone height and width with a graft improves implant stability and helps ensure predictable osseointegration.
In some cases a graft can be placed at the time of extraction to preserve the ridge for future implant placement, while other situations require a separate augmentation procedure performed months before implant surgery. The decision to graft and the chosen technique depend on clinical exam, three-dimensional imaging such as CBCT, and a comprehensive treatment plan tailored to the patient’s restorative goals. A staged approach provides the greatest control when large or complex defects exist.
Graft materials fall into several categories: autografts (patient’s own bone), allografts (donor human bone), xenografts (animal-derived bone), and alloplasts (synthetic bone substitutes). Autografts are osteogenic and integrate well but require a separate harvest site, while allografts and xenografts avoid additional surgery and provide a reliable scaffold for new bone formation. Synthetic materials can be highly controlled in composition and porosity and are often used when donor tissue is not indicated.
Each material has advantages and limitations related to biological activity, resorption rate, and handling characteristics, so selection is individualized for the defect and clinical objectives. Surgeons may combine materials or use biologically active adjuncts and membranes to support regeneration and protect the graft. Thorough discussion with the treating clinician ensures the chosen material aligns with the patient’s needs and the planned restorative sequence.
A sinus lift, also called a sinus augmentation, is a grafting procedure performed in the upper posterior jaw to increase bone height beneath the maxillary sinus. It is typically recommended when there is insufficient vertical bone to place dental implants in the upper back teeth due to sinus pneumatization or previous bone loss. During the procedure the sinus membrane is gently elevated and graft material is placed to build up the bone in that area.
Sinus lifts can be done as a separate augmentation before implant placement or simultaneously with implant installation when primary stability is achievable. Careful preoperative imaging and surgical planning are essential to evaluate sinus anatomy, membrane integrity, and the amount of graft needed. With proper technique, a sinus lift creates a predictable environment for stable implant support in the posterior maxilla.
A bone graft procedure begins with a thorough clinical evaluation and three-dimensional imaging to assess the defect and plan the augmentation. On the day of surgery local anesthesia with or without sedation is used to ensure patient comfort, and an incision is made to expose the deficient bone. The graft material is placed into the prepared site and often covered with a membrane to stabilize the graft and guide healing before the soft tissue is sutured closed.
Smaller ridge preservation grafts may be completed at the time of extraction, while larger augmentations require more extensive access and careful closure to protect the graft during healing. The use of biologically active matrices, membranes, and precise suturing techniques helps reduce the risk of exposure or contamination. Postoperative follow-up includes monitoring for proper healing and scheduling any additional restorative procedures when the graft has matured.
After a bone graft patients can expect some swelling, mild-to-moderate discomfort, and limited activity for a few days; these symptoms are typically managed with prescribed or over-the-counter medications and cold compresses. Oral hygiene instructions are provided to protect the surgical site, and patients are advised to avoid strenuous activity, smoking, and forceful rinsing until cleared by the clinician. Follow-up visits are scheduled to monitor healing and to remove sutures if necessary.
Dietary modifications such as soft foods and avoiding chewing directly over the grafted area are recommended during the initial healing period. If antibiotics or antimicrobial rinses are prescribed, patients should follow the full course to reduce infection risk. The surgeon will use clinical exams and imaging to determine when the graft has integrated and when it is safe to proceed with implant placement or other definitive restorations.
As with any surgical procedure, bone grafting carries risks including infection, prolonged swelling, graft exposure, and delayed or incomplete integration of the graft material. Specific procedures, such as sinus lifts, also carry the potential for sinus membrane perforation or sinus-related complications, which the surgeon will evaluate and address during the operation. Nerve injury is uncommon but possible in grafts near major neurovascular structures, so careful planning is essential to minimize this risk.
Risk is reduced by selecting appropriate candidates, using sterile technique, and following postoperative instructions closely, including smoking cessation when indicated. Early recognition and prompt management of complications improve outcomes, so patients should report unusual pain, persistent drainage, fever, or changes in sensation to the office immediately. Most complications are manageable and do not preclude eventual successful rehabilitation when handled promptly.
Bone grafts provide the structural support necessary for implants to achieve stable, long-term osseointegration by restoring adequate bone volume and density. Implants placed into well-augmented sites distribute chewing forces appropriately and reduce the likelihood of implant failure caused by inadequate primary stability or insufficient surrounding bone. Augmentation also helps preserve or restore facial contours, which contributes to both functional and esthetic success of implant-supported restorations.
Planning for bone grafting is integrated into the overall implant treatment sequence to ensure the site is ready for predictable implant placement and prosthetic restoration. Advanced imaging such as CBCT and digital planning tools guide the timing and extent of grafting so that implants can be placed in an optimal position. Coordinated care between the surgeon and restorative dentist maximizes the long-term prognosis of the implant-supported tooth or bridge.
The healing timeline after a bone graft varies by graft type, location, and the size of the defect, but most grafts require several months to mature before an implant can be placed. Smaller ridge preservation grafts may allow implant placement in three to four months, while larger or more complex augmentations—such as block grafts or extensive sinus lifts—often require four to nine months for sufficient bone remodeling. The clinician evaluates healing with periodic clinical exams and imaging to confirm graft integration.
In some clinical situations an implant can be placed at the same time as the graft if primary stability is achievable and the surgical plan supports a combined approach. The decision to stage implant placement or to perform simultaneous grafting and implantation is based on long-term restorative goals, bone quality, and the predictability of achieving stable implant fixation. Your surgeon will recommend the safest timing to optimize both graft and implant success.

Have questions or need to book your next appointment?
Our friendly staff at M. Kurt Berky, DDS, PC is ready to assist. Whether by phone or our online contact form, contacting us is simple and convenient. Start your journey to a healthier, brighter smile today by reaching out to our office.